If a patient with cancer arrives confused, dehydrated, and constipated—and the ECG shows a shortened QT—think hypercalcemia of malignancy (HCM). I’ve coached many students through this exact scenario. This guide gives you a clear, NGN-ready roadmap: fast pathophysiology, prioritized nursing diagnoses with SMART outcomes, and step-by-step interventions with rationales tailored to oncology care (bisphosphonates/denosumab, calcitonin, and aggressive hydration). You’ll know what to assess first, how to protect from cardiac/renal complications, and how to teach patients and families.
Studying multiple electrolytes? Read our master hub:
The Ultimate Guide to Electrolyte Imbalances - frameworks, tables, and 20+ NGN micro-cases.
If you want the complete, up-to-date breakdown of AI for NCLEX prep + nursing school—with independent university study metrics—use this master guide: The Ultimate Guide to AI for NCLEX Preparation and Nursing School.
🎯 Free NCLEX quiz!
Test your knowledge - new quizzes added weekly!
Cross-reference for mastery: Pair this with our core calcium pages for quick differentials:
• Hypercalcemia Nursing Care Plan (2025)
• Hypocalcemia Nursing Care Plan (2025)
• Primary Hyperparathyroidism Nursing Care Plan (2025)
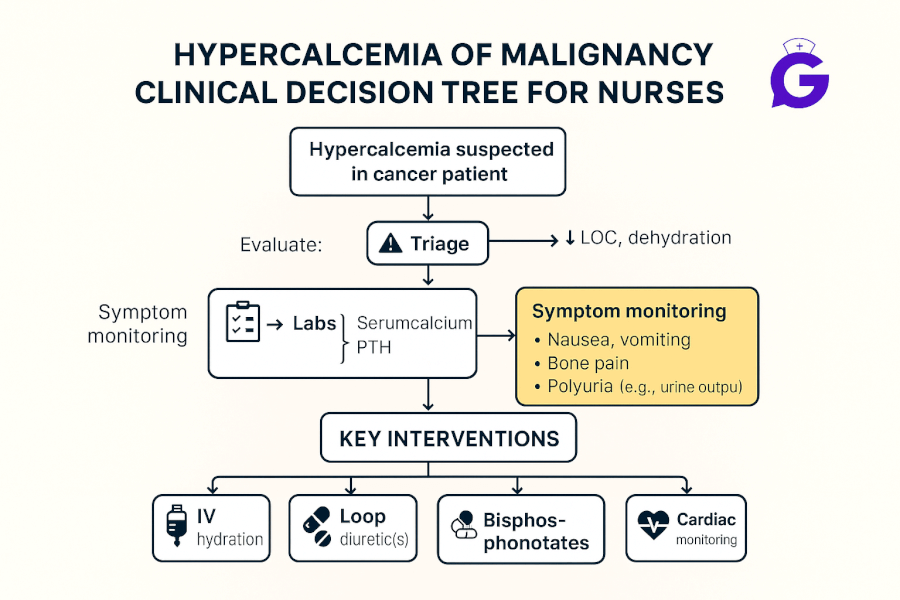
Pathophysiology of Hypercalcemia of Malignancy
HCM is driven by tumor-related mechanisms that raise serum calcium, commonly PTH-related peptide (PTHrP) secretion, osteolytic bone metastases, or excess 1,25-(OH)₂-vitamin D (e.g., some lymphomas). The result is increased bone resorption and renal reabsorption of calcium, causing neuromuscular depression, GI slowing (constipation), polyuria/dehydration, and cardiac changes (shortened QT, dysrhythmias). Initial management is isotonic IV fluids, rapid-acting calcitonin, and longer-acting antiresorptives (IV bisphosphonates or denosumab) while treating the underlying cancer. See concise overviews at the NCI and NCBI/StatPearls: National Cancer Institute, NCBI Bookshelf.
Nursing Care Plans for Hypercalcemia of Malignancy
Use these prioritized nursing diagnoses to individualize care. Values and orders vary—always follow provider protocols and your institution’s guidelines.
Nursing Diagnosis: Risk for Deficient Fluid Volume
| Category | Details |
|---|---|
| Related to | Osmotic diuresis and impaired concentrating ability from hypercalcemia; anorexia/nausea |
| As evidenced by | (Risk factors) Polyuria, dry mucosa, orthostasis, low urine specific gravity, rising BUN/Cr, poor intake |
| Desired Outcomes | UO ≥ 0.5–1 mL/kg/hr; VS stable; weight trending up to baseline; labs show improving calcium and renal function within 24–48 hrs. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Start **isotonic IV fluids** per order; maintain strict I&O and daily weights. | Volume repletion enhances renal calcium excretion and protects kidneys. |
| Avoid **calcium-containing IV fluids** (e.g., Lactated Ringer’s) in significant hypercalcemia. | Prevents additional calcium load while levels are high. |
| Monitor BMP, ionized Ca²⁺, and ECG; notify for rapid rises or symptoms. | Guides therapy and detects evolving dysrhythmias or renal injury. |
Nursing Diagnosis: Acute Confusion
| Category | Details |
|---|---|
| Related to | Elevated serum calcium and dehydration causing altered cerebral function; cancer-related fatigue |
| As evidenced by | Disorientation, poor attention, impaired judgment, family report of acute change |
| Desired Outcomes | Remains oriented ×4 and free from injury within 24–48 hrs; CAM negative; safe environment maintained. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Institute fall precautions, frequent reorientation, and low-stimulus environment. | Reduces injury risk while cognition improves with treatment. |
| Administer **calcitonin** for rapid calcium lowering and prepare for **IV bisphosphonate or denosumab** per oncology order. | Calcitonin acts quickly but transiently; antiresorptives provide sustained control in HCM. |
| Screen for reversible contributors (thiazides, calcium/vitamin D supplements) and hold if appropriate. | Prevents iatrogenic elevation of calcium. |
🥇Voted #1 Nursing Study Tool.
Personalized AI Tutor + Instant Answers to All Your Questions. 100% Money Back Guarantee!
Nursing Diagnosis: Risk for Decreased Cardiac Output (dysrhythmias)
| Category | Details |
|---|---|
| Related to | Shortened QT interval and altered myocardial conduction from elevated calcium |
| As evidenced by | (Risk state) Shortened QT on ECG, palpitations, dizziness, oncology diagnosis with HCM |
| Desired Outcomes | Maintains stable rhythm; no syncope; ECG trends normalize as calcium corrects; reports no chest discomfort. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Continuous ECG monitoring in moderate–severe HCM. | Detects dysrhythmias early and guides escalation. |
| Trend electrolytes (K⁺, Mg²⁺, phosphate) and replace per protocol. | Electrolyte imbalances compound dysrhythmia risk. |
Nursing Diagnosis: Deficient Knowledge (oncology-specific calcium management)
| Category | Details |
|---|---|
| Related to | New diagnosis of HCM; unfamiliarity with hydration/medications and red-flag symptoms |
| As evidenced by | Questions about drugs (calcitonin, zoledronic acid, denosumab), diet/supplements, and when to seek care |
| Desired Outcomes | Patient/family teach back hydration targets, medication purpose/timing, and return precautions before discharge. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Explain medication sequence: fluids → calcitonin (rapid, short-term) → antiresorptive (slower, sustained). | Sets expectations for symptom relief and lab trajectory. |
| Provide written precautions: worsening confusion, severe constipation, palpitations, decreased urine, uncontrolled nausea/vomiting. | Prompts timely escalation to prevent renal/cardiac complications. |
Frequently Asked Questions (FAQ)
What is the first-line treatment for hypercalcemia of malignancy?
Isotonic IV fluids to correct dehydration and promote calciuresis, often alongside calcitonin for rapid effect and IV bisphosphonate or denosumab for sustained lowering.
Which drug lowers calcium the fastest?
Calcitonin acts within hours but is short-lived; zoledronic acid or denosumab take longer to work but provide durable control in HCM.
Can I use Lactated Ringer’s in severe hypercalcemia?
Avoid calcium-containing fluids (e.g., LR) until calcium normalizes—use 0.9% Normal Saline or other isotonic non-calcium options per order.
Why is HCM dangerous for the heart and kidneys?
High calcium shortens QT (dysrhythmias) and causes polyuria/dehydration, which can precipitate AKI—hence the focus on ECG, I&O, and BMP trending.
Further Reading
- Hypercalcemia Nursing Care Plan (2025)
- Hypocalcemia Nursing Care Plan (2025)
- Primary Hyperparathyroidism Nursing Care Plan (2025)
- NGN Med-Surg Case Studies: Physiological Adaptation
- ABG Interpretation: 15 Practice Cases
References
- National Cancer Institute (NCI): Cancer Information
- NCBI Bookshelf (NIH): Hypercalcemia of Malignancy overviews (StatPearls/Endotext)
Download our free printable Fluids & Electrolytes cheat sheet. Enter your email below and we'll send it right over.