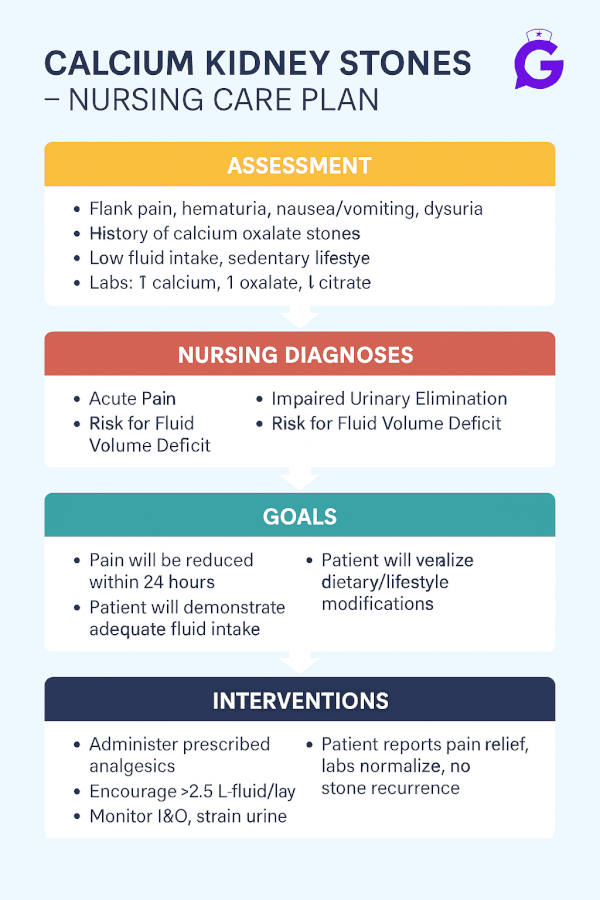
Renal colic is one of those cases that can rattle even seasoned students—sudden flank pain, nausea, hematuria, and a patient who can’t get comfortable. In this NGN-ready guide, I’ll walk you through a clear nursing care plan for calcium kidney stones (most stones), focused on what improves outcomes fast: pain control, hydration, obstruction monitoring, and infection prevention—plus what to teach so patients avoid recurrence. You’ll get prioritized nursing diagnoses with SMART outcomes, and step-by-step interventions with rationales you can use today in pre-conference, simulation, and clinical.
Studying multiple electrolytes? Read our master hub:
The Ultimate Guide to Electrolyte Imbalances (2025) - frameworks, tables, and 20+ NGN micro-cases.
🎯 Free NCLEX quiz!
Test your knowledge - new quizzes added weekly!
Table of Contents
- Pathophysiology of Calcium Kidney Stones
- Nursing Care Plans (Diagnoses, Outcomes, Interventions & Rationales)
- FAQs
- Further Reading
- References
Pathophysiology of Calcium Kidney Stones
Calcium oxalate and calcium phosphate stones form when urine becomes supersaturated with stone-forming salts and lacks enough inhibitors (e.g., citrate). Key drivers include low urine volume (dehydration), hypercalciuria (e.g., hyperparathyroidism), hyperoxaluria, low citrate, high sodium intake, and prolonged immobility. As a stone migrates into the ureter, ureteral spasm/obstruction triggers severe colicky pain, hydronephrosis risk, and sometimes infection. First-line management typically includes analgesia, antiemetics, hydration, urine straining, and monitoring for fever, solitary kidney, rising creatinine, or uncontrolled pain that warrant urgent escalation. For overviews on causes and prevention, see the NIDDK (NIH) and practice guidance from the American Urological Association.
Cross-reference the calcium mini-cluster to master the differentials and etiologies:
• Hypercalcemia Nursing Care Plan (2025)
• Hypocalcemia Nursing Care Plan (2025)
• Primary Hyperparathyroidism Nursing Care Plan (2025)
• Hypercalcemia of Malignancy Nursing Care Plan (2025)
Nursing Care Plans for Calcium Kidney Stones
Use these prioritized nursing diagnoses with outcomes and rationales to individualize care.
Nursing Diagnosis: Acute Pain (renal colic)
| Category | Details |
|---|---|
| Related to | Ureteral spasm and increased intraluminal pressure from obstructing stone |
| As evidenced by | Severe flank pain radiating to groin, restlessness, nausea/vomiting, hematuria, guarding |
| Desired Outcomes | Reports pain ≤ 3/10 within 60–90 minutes of treatment; able to ambulate and tolerate oral intake. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Administer prescribed analgesics (e.g., NSAID and/or opioid) and antiemetics; reassess pain and nausea on a timed schedule. | Relieves colicky pain and permits hydration/ambulation; reassessment confirms efficacy and safety. |
| Encourage hydration per order; initiate IV fluids if unable to tolerate PO. | Adequate volume supports urine flow, may aid stone passage, and reduces further supersaturation. |
| Apply non-pharmacologic strategies (heat to flank, guided breathing, position of comfort). | Adjuncts reduce muscle spasm perception and anxiety, complementing medication therapy. |
Nursing Diagnosis: Impaired Urinary Elimination (obstruction)
| Category | Details |
|---|---|
| Related to | Mechanical obstruction from ureteral calculus with edema/spasm |
| As evidenced by | Reduced urine output, urgency, frequency, incomplete emptying, hematuria; imaging showing stone |
| Desired Outcomes | Urine output ≥ 0.5–1 mL/kg/hr; passes stone or has definitive urologic management; no post-obstructive AKI. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Maintain strict I&O; strain all urine; save any passed stone for analysis. | Tracks obstruction severity and enables metabolic workup (stone type informs prevention). |
| Monitor for red flags: fever, solitary kidney, rising creatinine, anuria, uncontrolled pain. | These require urgent provider notification and possible urologic decompression. |
| Administer alpha-blocker or antispasmodic therapy if prescribed (medical expulsive therapy). | Relaxes ureteral smooth muscle to facilitate passage of distal ureteral stones per provider plan. |
Nursing Diagnosis: Risk for Infection (urinary tract)
| Category | Details |
|---|---|
| Related to | Urinary stasis from obstruction; possible instrumentation |
| As evidenced by | (Risk state) Dysuria, cloudy/foul urine, fever/chills; positive UA pending culture |
| Desired Outcomes | Remains afebrile; UA improves; no progression to pyelonephritis or sepsis. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Assess for fever, CVA tenderness, dysuria; obtain UA/urine culture as ordered. | Early detection and organism identification guide timely therapy. |
| Start antibiotics per order if infection suspected; escalate urgently if obstructed and febrile. | Obstructed, infected systems can progress rapidly—require decompression and antibiotics. |
Nursing Diagnosis: Deficient Knowledge (prevention & recurrence reduction)
| Category | Details |
|---|---|
| Related to | Unfamiliarity with hydration, diet, and medication strategies; misunderstanding about calcium restriction |
| As evidenced by | Questions about fluids, sodium, calcium/oxalate intake, citrate, and stone analysis follow-up |
| Desired Outcomes | Patient/family teach back a prevention plan: fluids, diet, medications (if prescribed), and follow-up testing. |
Nursing Interventions and Rationales
| Intervention | Rationale |
|---|---|
| Teach hydration targets (aim for pale-yellow urine); spread fluids throughout the day. | Higher urine volume lowers supersaturation and stone formation risk. |
| Clarify diet basics: **do not severely restrict dietary calcium**; moderate sodium; limit high-oxalate foods if calcium-oxalate stone; increase fruits/vegetables (citrate sources). | Normal calcium intake binds oxalate in the gut; high sodium increases calciuria; citrate inhibits crystallization. |
| Review meds if prescribed (e.g., thiazide, potassium citrate); reinforce adherence and lab follow-up. | Medication therapy targets the specific metabolic driver (hypercalciuria, hypocitraturia). |
Frequently Asked Questions (FAQ)
What is the priority intervention for renal colic from a suspected stone?
Rapid pain control and hydration. Treat pain (often NSAID ± opioid), control nausea, initiate fluids, and assess for red flags (fever, anuria, solitary kidney, rising creatinine).
Should patients cut out calcium to prevent stones?
No. Maintain normal dietary calcium unless a provider advises otherwise. Severe restriction can increase intestinal oxalate absorption and raise stone risk (see NIDDK).
When is urgent urology consult needed?
Suspected obstructed infection (fever + obstruction), anuria, solitary kidney, uncontrolled pain, or worsening renal function—these require immediate escalation.
Further Reading
- Hypercalcemia Nursing Care Plan (2025)
- Hypocalcemia Nursing Care Plan (2025)
- Primary Hyperparathyroidism Nursing Care Plan (2025)
- Hypercalcemia of Malignancy Nursing Care Plan (2025)
- NGN Med-Surg Case Studies: Physiological Adaptation
- ABG Interpretation: 15 Practice Cases
References
- National Institute of Diabetes and Digestive and Kidney Diseases (NIH): Kidney Stones
- American Urological Association: Kidney Stone Guidelines (overview)
Download our free printable Fluids & Electrolytes cheat sheet. Enter your email below and we'll send it right over.